
Last week the review from the National Mental Health Commission (NMHC) was finally released. The report was an important review, covering all mental health care services in Australia. Our Health Minister (actually, two of them) sat on the report, prompting us to make an FOI request to which the Government replied that we must pay a hefty sum of $1744.92 to process our request. We gave up and waited until last week when leaks of the report started appearing. At first the leaks trickled information out from the first chapter (via the ABC), but within days the full report was leaked (to Crikey.com). By midday on the same day the NMHC officially announced that the report was public.
There’s a lot to say about the findings of the review, which we will get to in the weeks ahead. For now we will focus on one aspect of the report which has dominated the debate so far: funding. The NMHC Report recommends (page 10, Rec 7) that $1 billion in funding should be re-directed away from acute hospital-based mental health care to community-based programs. Psychiatrists are opposed to the plan and almost immediately we started hearing deep concerns (on our Facebook group) from people who have accessed hospital-based mental health care. It is hardly news here in Australia that people often struggle to get admitted when they really need help and feel abandoned when they are discharged too early. The problem seems to be that mental health care in hospitals is already struggling to cope with limited funding. As one person eloquently put it:
The last time i went to a psychiatric emergency centre my first thought wasn’t “Gee this place would run much more efficiently if they stripped a billion dollars out of the sector”
As it turns out that the recommendation to pull hospital funding is not the fault of the Commission. Professor Alan Fels pointed out that the Terms of Reference (ToRs) that the Commission had to abide by, specified that they must work within the existing “funding envelope”. In effect, the Commission was told not to recommend any additional funding for mental health care.
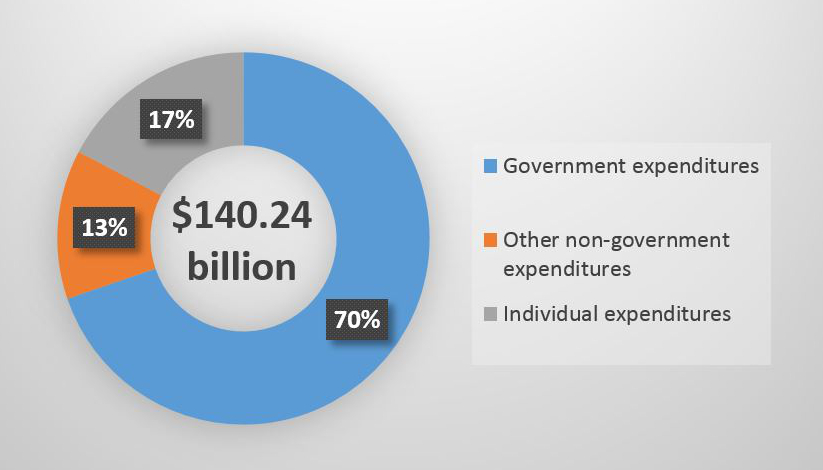 That made me curious about the expenditure figures, so I took a closer look. For the 2011-2012 period covered by the NMHC Report the total health expenditure is estimated at $140.24 billion (see AIHW report). As can be seen by the pie-graph on the left (note: you can click on it to make it larger) the vast majority of health funding is sourced from Government, followed by individuals, then non-government bodies. It’s a sizeable amount of money, but the question is how much of it actually goes to mental health care?
That made me curious about the expenditure figures, so I took a closer look. For the 2011-2012 period covered by the NMHC Report the total health expenditure is estimated at $140.24 billion (see AIHW report). As can be seen by the pie-graph on the left (note: you can click on it to make it larger) the vast majority of health funding is sourced from Government, followed by individuals, then non-government bodies. It’s a sizeable amount of money, but the question is how much of it actually goes to mental health care?
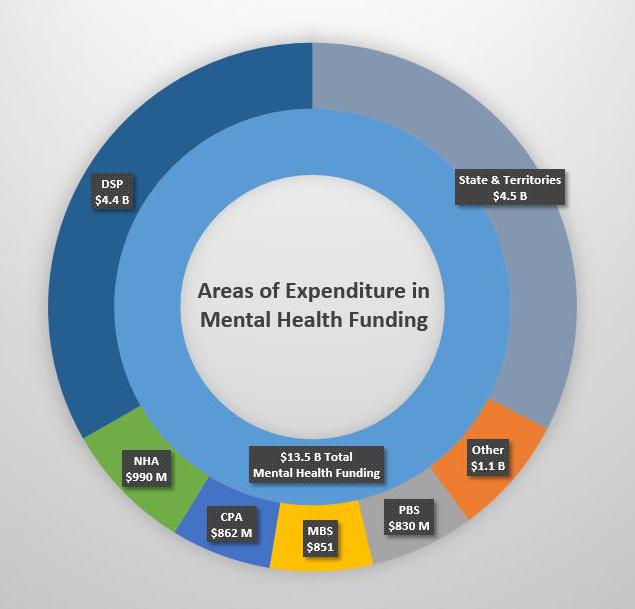 The NMHC Report states that the combined Commonwealth, state, and territory funding for mental health care amounts to an estimated $13.52 billion (see Vol. 4, page 4). As can be seen on the right, approximately one third of the funding comes from the states and territories; and another third of the funding goes towards the Disability Support Pension (DSP). These figures raise some important questions about what proportion of the funding is directed to treatment of mental health disorders. As can be seen by the pie-graph, a relatively small fraction of that funding goes to medication (via the PBS at 6.1%) and treatment services delivered under Medicare (via the MBS at 6.3%). The current picture of mental health care funding is that much of it is committed to various services and programs which do not provide treatment. Although such programs are very much in need by those living with a mental health condition, it is important to appreciate how little of our funding actually goes to providing therapy, medication, and so on.
The NMHC Report states that the combined Commonwealth, state, and territory funding for mental health care amounts to an estimated $13.52 billion (see Vol. 4, page 4). As can be seen on the right, approximately one third of the funding comes from the states and territories; and another third of the funding goes towards the Disability Support Pension (DSP). These figures raise some important questions about what proportion of the funding is directed to treatment of mental health disorders. As can be seen by the pie-graph, a relatively small fraction of that funding goes to medication (via the PBS at 6.1%) and treatment services delivered under Medicare (via the MBS at 6.3%). The current picture of mental health care funding is that much of it is committed to various services and programs which do not provide treatment. Although such programs are very much in need by those living with a mental health condition, it is important to appreciate how little of our funding actually goes to providing therapy, medication, and so on.
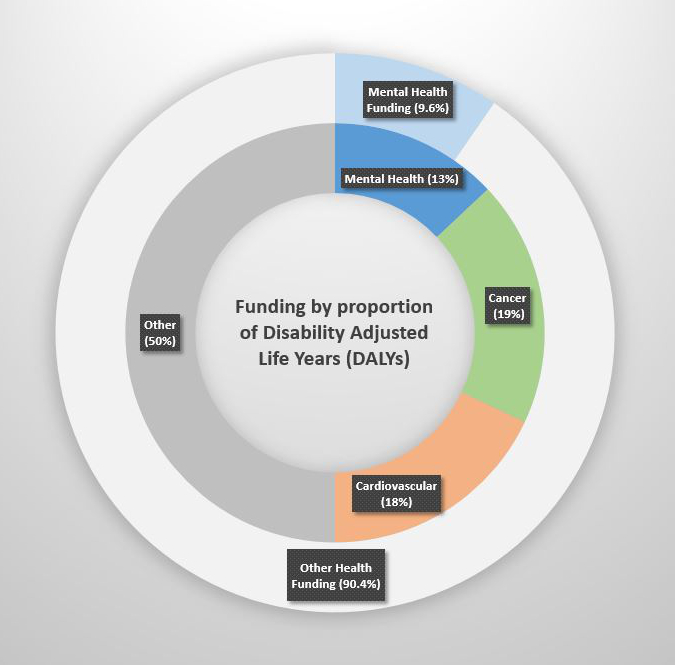 Looking at these figures we can see that only 9.6% of the $140.24 billion directed to health actually reaches mental health. When we compare that to figures such as the burden of disability there is an obvious mismatch. Mental health disorders have been calculated to represent 13% of the years of life lost by comparison to cancer (19%) and cardiovascular disease (18%). Put simply, the scale of our investment on mental health does not align with the size of the issue. One might argue that 9.6% and 13% is not that big of a difference, however, when we look at those percentages in terms of actual funding, that’s a difference of nearly $5 billion. And if we repeat the calculations by removing non-treatment funding (such as the DSP), then the figure sits at just 6.5%, or an additional $9.1 billion we should be directing to mental health care.
Looking at these figures we can see that only 9.6% of the $140.24 billion directed to health actually reaches mental health. When we compare that to figures such as the burden of disability there is an obvious mismatch. Mental health disorders have been calculated to represent 13% of the years of life lost by comparison to cancer (19%) and cardiovascular disease (18%). Put simply, the scale of our investment on mental health does not align with the size of the issue. One might argue that 9.6% and 13% is not that big of a difference, however, when we look at those percentages in terms of actual funding, that’s a difference of nearly $5 billion. And if we repeat the calculations by removing non-treatment funding (such as the DSP), then the figure sits at just 6.5%, or an additional $9.1 billion we should be directing to mental health care.
Now if we return to the recommendations of the NMHC Report, the question is where we can find $1 billion in funding for community-based mental health care? It seems pretty obvious from the above figures that we are not committing nearly enough funding to mental health care in the first place. Reshuffling the same sparse funding amounts to redistributing the crisis. If Australia can afford $12 billion for 58 more F-35 Joint Strike Fighters then surely we can afford just $1 billion for community-based mental health care. Cant we?

Pauline Miles
My experience is that we do need more money out into mental health care in the public systems. From my own experience there are not enough psychologists in the public system where it is free for people who can’t afford the luxury of going to a private psychologist. Oh yes we have the mental health care plan that allows for 6 to 10 sessions. This is where the issues lie. I know that I would not want to open Pandora’s box only to know that I would not get the treatment idea that once I had opened up, after a few appointments, my deep pain to know that i only had a few appointments to work with a practitioner, knowing that I would be left in the middle of therapy because I could not afford the cost of further treatment for my individual needs. It took a lifetime of abuse to make and you should not have a time limit placed on therapy of this nature. It is a very dangerous practice to open Pandora’s box and leave people hanging on a cliff edge.
It should not be time limited, it should be as long as it takes. We have such an unfair system where people who have the wealth can afford good treatment and those of us who are on DSP or low incomes can’t afford the necessary treatment we need to keep our mental health and out our general well-being in good shape. We need more services that are affordable to the poor and that will not happen if money is not put into the already, burden public system. So people can access therapy. Community care is also in need of a boost in funding but you can’t rob Peter to pay Paul.