
Next week the Australian Psychological Society (APS) will release a Green Paper for consultation with their members about the Medicare Benefits Schedule (MBS) Review. The current Medicare system faces a number of problems. To name just a few: people in distress are required to accept the label of a mental disorder to access therapy, and once they begin, the amount they get back from Medicare varies considerably and doesn’t last long enough. Change is long overdue, so the Government is looking to the APS for suggestions on how to improve the system.
One of the biggest concerns I’ve been hearing lately is about the three-tiered system which was recently proposed by the APS during the MBS Review. Conflict over the three-tiered plan erupted to the point that it made national headlines. You can read some of my commentary on this below that newspaper article and on Twitter. However, I’ve been thinking that it might be helpful for everyone to take a moment to go over some of my commentary in point form ahead of this Green Paper being released on Monday. That’s why I wrote this brief piece you’re reading right now.
First, here’s the APS three tiered plan which caused the row: https://www.psychology.org.au/getmedia/5ee546ee-7a78-4807-a404-45d0d12adca7/2018-APS-submission-Better-Access-following-presentation-aug.pdf
My points of critique to that plan are as follows:
- This submission was released to APS members the day after the consultation closed, leaving no space for feedback. It also came just shortly after APS membership renewal.
- Members of the APS were not invited to contribute to the submission, or provide any feedback, prior to submission being delivered to Government.
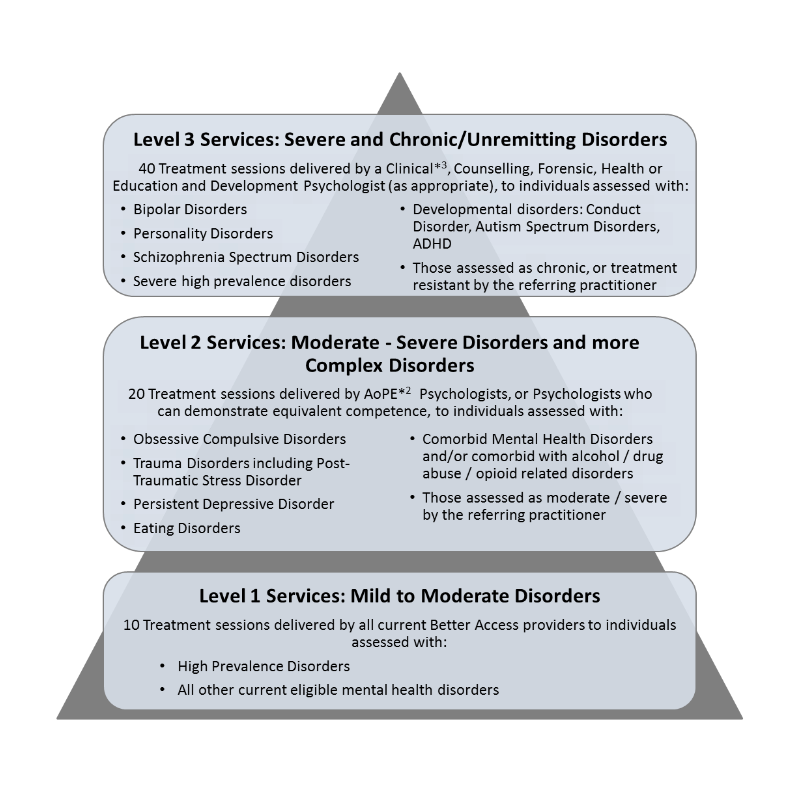
- Page 6 of the APS submission shows a tiered model of services. Previously the APS has claimed that the tiered model is unfair and that the government chose it. It is worth noting that a three-tiered model similar to this one was offered to the APS College of Counselling Psychologists around 2008 and subsequently rejected for being unfair and not resolving the issue.
- Non-psychologist mental health practitioners are positioned at the bottom tier – ten sessions with mild-to-moderate disorders. This is the current system and it indicates the APS excluding other practitioner groups from changes they have in mind.
- The APS submission makes no attempt to challenge the ‘focused psychological strategies’ (FPS) construct. FPS interventions are in fact identical to those classed as ‘psychological therapy’ – we are all ethically bound to use evidence-based interventions for our work. Patients can use same referral for both items.
- Should the patient enter at level 1 and require more than ten visits of care, then this model would see them referred to a different practitioner to start all over again – unless they start therapy with an endorsed psychologist.
- The model makes no mention of MBS rebates for each level. If there is a higher MBS rebate for higher levels, then the patient may receive less/more support for the same services. In terms of eligible disorders, the question is whether a patient with mild to moderate depression deserves less support from Medicare per session than one with a personality disorder? We must remember that the MBS rebate belongs to the patient, not the practitioner.
- The APS model cobbles together severity, chronicity, complexity, and prevalence as though they can be positioned along an axis where they can slot practitioner groups into categories. This appears to be about marketing practitioner groups by disorder.
- Imagine the GP consultation. You have 15 minutes or so to help them make a quick call on where to position you on this model. Depending on their call, you could get 10 sessions, 20 sessions, or 40 sessions. Rate of support per session might be really low or high.
- Page 7 shows a table of proposed revisions to MBS items. The top row item for GP referral “Allow the referring practitioner to have the option to refer to appropriately qualified psychologists for a full assessment and completion of a mental health treatment plan.” Page 8 clarifies what the APS meant by “appropriately qualified psychologists”. They are referring specifically to clinical psychologists. This item only allows the GP to refer to a clinical psychologist “for assessment, opinion and report, or ongoing management”.
- Note the asterixes with the text on the pyramid model on page 6, which are defined on page 5 under ‘explanatory notes’. Point 3 on this list of notes is identical in structure to the language used in the original 2006 submission leading to the model we have now which elevates clinical psychology above all other relevant domains of mental health care. The language here that other areas “may also have additional competencies for specific disorders” lends itself to a false impression that clinical psychologists always have additional competencies across the full range of disorders.
I lapsed my APS members a few years ago, when I realised they weren’t representing what I do in practice or the best interests of the people I work with in the community. It really didn’t make any difference whether I remained a member or not. My clients will continue to suffer the bad advice being delivered to our politicians who honestly do not know any better. Personally, I find this whole drama unfolding before us a very sad state of affairs. I’ll leave it up to the rest of you who are APS members to respond. Good luck. You’re probably going to need it! My focus now is on other matters.
PLEASE NOTE: This is at times a highly charged topic and comments on this thread are moderated. If you are speaking as a mental health care professional, then please identify yourself by name to maintain ethical standards and professional respect. I would like to keep the discussion positive and focused on how we can improve the Medicare system to benefit the community. You may be asked to support your view. However, elitism and disrespect has no place here. Thanks in advance.
