

In the Medicare system, the Better Access to Mental Health Care refers patients with an eligible disorder to see a therapist for evidence-based psychological care. Depending on your choice of provider, you may receive as little back from Medicare as $74.80 or as much as $124.50 for a one hour appointment. Yet all eligible providers deliver services from the same short list of evidence-based approaches.
For over a decade, inequities in the level of support provided by Medicare have raised public objections and tensions between mental health providers. Those who support the status quo are typically practitioners favoured by the scheme – mainly clinical psychologists. Their argument usually goes along the lines that the services they provide are superior and they deserve more money for their training. Despite decades of research, the superiority of any one practitioner group over the others has not been established.
The question of differences between service providers hinges on whether those differences are sufficient or not. In this short piece, I will explain why those purported differences are insufficient to warrant a different Medicare rebate. All providers in the scheme should meet sufficiently high standards to deliver evidence-based psychological care – and patients should be given equitable support from Medicare when they receive it.
You’ll find a wide range of skills, knowledge, and ability within any practitioner group. Some would argue that the quality of therapists varies as much within each practitioner group as it does between them. Any given therapist has their strengths and deficits, so trivial differences between mental health care providers generally don’t warrant distinctions being made at the policy-level. Therefore, if we are going to establish an approachable model of care for patients to access, the focus should be on identifying where there are large differences in the quality and outcomes of therapy. Research consistently finds that the training background of a psychotherapist does very little to produce better or worse outcomes (Anderson et al., 2009; Beutler et al., 2004; Okiishi et al., 2006; Okiishi et al., 2003; Wampold & Brown, 2005). In measurable terms, the purported differences between practitioner groups are rarely detectable and certainly not large by any stretch of the imagination.
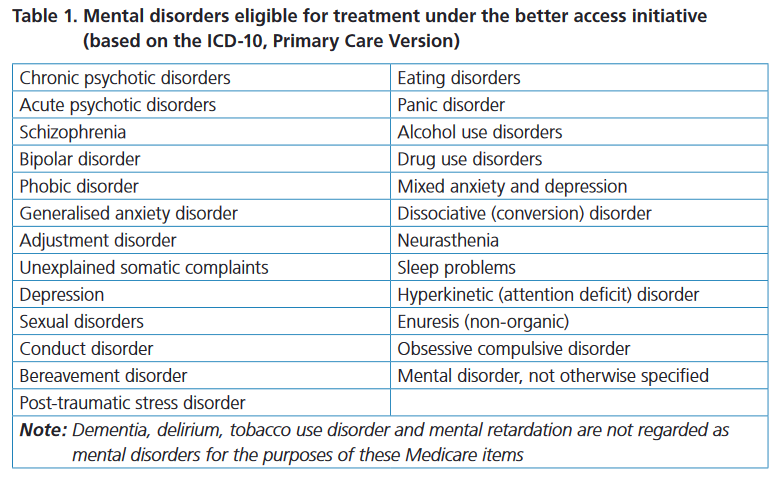
If we are going to differentiate the categories of practitioner, then it should also matter whether we are making any relevant distinctions. In the Medicare system, all patients referred to psychological care must have an eligible disorder (see table). Once they are given a referral, the patient is free to use their referral to access any eligible provider in the scheme. That therapist must then provide an evidence-based therapy appropriate for the treatment of that disorder. There’s no scope in the Medicare system for a provider to deliver therapies which are not evidence-based or to work beyond the 6 to 10 session framework. Similarly, there are no functional distinctions between the classes of intervention we use under the various MBS item numbers in the scheme either (Carey, Rickwood, & Baker, 2010). In other words, there’s no practical or substantive distinction to be made about the type of services being provided.
It’s worth bearing in mind that there’s no restricted form of psychotherapy reserved exclusively for clinical psychologists. The types of psychological approaches which are used by clinical psychologists are actually no different to those used by other mental health care professionals. In fact, if one were to deliver therapy in a markedly different way, that would raise some serious concerns about treatment fidelity. As a case in point, the prerequisite training for nationally accredited training in CBT is open to “psychology, nursing, medicine, social work, education, occupational therapy, counselling”. We see the same pattern in national accreditation standards for IPT which are open to “psychologists, clinical psychologists, social workers, psychiatrists, nurses, occupational therapists, psychotherapists, general practitioners etc.” For those new to this subject, CBT and IPT are the two main evidence-based approaches recommended by the Better Access scheme. A quick check of the studies cited by the most up to date APS list of evidence based psychological interventions confirms that the sample of therapists participating in these studies come from a broad range of practitioner groups
Claims that there are differences between practitioner groups are bold, and consequently, any claim of that kind ought to be well-established. As in other domains outside of the mental health sector, that means backing up a claim with solid research and a stable pattern of relatively consistent results. In the discipline of Psychology, we are after all, scientist-practitioners. Therefore, we should hold ourselves to high standards about evidence. Instead, what we typically find is that the purported differences are made on the basis of speculation, theoretical grounds, or by appeal to anecdote. There’s every chance claims of that kind do not amount to any real differences in practice. Public policy should not be based on information which exposes us to genuine risks of bias, elitism, discrimination, or corruption.
As much as we might wish for there to be research showing that postgraduate psychology degrees make us better at working with more severe and complex issues, data from research simply does not support that claim. What it does show are relatively modest improvements (d = 0.04 per year of additional training) but only for less distressed client populations (Owen et al., 2016). However, that conclusion doesn’t fit the narrative of superior outcomes for working with more severe, complex, and chronic mental health issues. So unfortunately, professional lobby groups continue to ignore that point when trying to make their case for a system that favours their particular group.
The ultimate test is whether policy is in the public interest. The needs of people who turn to us for care are paramount, especially in mental health care. How could it possibly be fair and equitable for patients to have different rates of Medicare support depending on who they see? It restricts consumer choice when Medicare offers less support for the same therapy. In the end, the only thing that really should matter here is whether the system serves the interests of distressed people reaching out for help. Personally, I can see no clear benefit to consumers in having a multi-tiered system. If they meet the entry criteria to get support via Medicare, then their choice of eligible provider should be respected and adequately supported. Person-centred care still matters, doesn’t it?
In summary, the purported differences between mental health care providers in the scheme appear to be trivial and irrelevant. There’s no practical distinction made about the type of service provided and the approved list of evidence-based therapies are not exclusive to clinical psychology. There’s no well-established data showing that clinical psychologists work with a different client population in private practice, or that they produce better outcomes in the Medicare scheme. Ultimately there appears to be no public interest case. A tiered model naturally restricts consumer choice and results in additional financial inequities. In the context of recent discussions about the MBS Review, there’s insufficient basis to argue for a tiered approach. Instead, we should be looking to a standard rate. There’s no reason why we cannot develop professionally-neutral criteria to identify suitably qualified mental health care providers in the scheme, for the sake of public interest, evidence-based practice, and good quality person-centred care.
References
Anderson, T., Ogles, B. M., Patterson, C., Lambert, J. E., & Vermeersch, D. A. (2009). Therapist effects: Facilitative interpersonal skills as a predictor of therapists success. Journal of Clinical Psychology, 65(7), 755-768.
Beutler, L. E., Malik, M., Alimohamed, S., Harwood, T. M., Talebi, H., Noble, S., et al. (2004). Therapist variables. In M. J. Lambert (Ed.), Bergin and Garfield’s handbook of psychotherapy and behavior Change. New York: Wiley.
Carey, T. A., Rickwood, D. J., & Baker, K. (2010). Tying up some loose ends: A rejoinder’s rejoinder. Clinical Psychologist, 14(2), 70-71.
Okiishi, J., Lambert, M. J., Eggett, D., Nielsen, L., & Dayton, D. D. (2006). An analysis of therapist treatment effects: Toward providing feedback to individual therapists on their clients’ psychotherapy outcome. Journal of Clinical Psychology, 62(9), 1157-1172.
Okiishi, J., Lambert, M. J., Nielsen, S. L., & Ogles, B. M. (2003). Waiting for supershrink: An empirical analysis of therapists effects. Clinical Psychology and Psychotherapy, 10, 361-373.
Owen, J., Wampold, B. E., Kopta, M., Rousmaniere, T., & Miller, S. D. (2016). As Good as It Gets? Therapy Outcomes of Trainees Over Time. Journal of Counseling Psychology, 63(1), 12-19.
Wampold, B. E., & Brown, G. S. (2005). Estimating variability in outcomes attributable to therapists: A naturalistic study of outcomes in managed care. Journal of Consulting and Clinical Psychology, 73(5), 914-923.
PLEASE NOTE: This is at times a highly charged topic and comments on this thread are moderated. If you are speaking as a mental health care professional, then please identify yourself by name to maintain ethical standards and professional respect. Comments from health practitioners who cannot be identified will not be published. In general terms, I would like to keep the discussion positive and focused on how we can improve the Medicare system to benefit the community. You may be asked to support your view. However, elitism and disrespect has no place here. Thanks in advance.